
What is Fetal Ejection Reflex (FER) and what does it have to do with my Pelvic Floor?
My body pushed my babies out involuntarily.
I didn’t push. At all.
Not only that, but for all four of my births I didn’t tear at all, AND I experienced transcendence of pain in all but one birth (and I know why that one was different… and I’ll share it with you!).
I’m sharing this because I truly believe that when birth is left alone, most womben will actually experience this, and furthermore, with a healthy pelvic floor, they may experience this as I did, with minimal pain, and instead in a state of euphoria.
What is Fetal Ejection Reflex (FER)?
And what does it have to do with my pelvic floor neurology?
FER, also known as the Ferguson reflex, in simple terms, is when the body involuntarily bears down to push the baby out during the second stage of labor, rather than having to intentionally push.
Typically what happens here is that the body, sensing the baby’s head or other presenting part pressing on the pelvic nerves, sends a signal to the brain which causes a release of oxytocin, causing some big contractions. It also sends a surge of adrenaline to mother and baby, bringing the laboring woman out of the endorphin rich “la-la labor land” that she was in during first stage and likely in the pause between first and second stage (the quietude). This causes the womban to feel the urge to get more upright, alert, and ready for being fully present as the baby emerges.
Our uterus has receptors in it for the hormone oxytocin, the hormone which many know of as the hormone of love and bonding, and, miraculously, also is the hormone responsible for uterine contractions! In late pregnancy, the uterine oxytocin receptors increase around 200x!
But what we need to understand is that there is a feedback loop between the brain and the pelvic and cervical nerves which causes the brain to release more oxytocin as well as other hormones, when the fetal head (or other presenting part) puts more pressure on those muscles and nerves, and stretch receptors of the cervix itself.
The cervix is the star of the show in the first stage of labor, and those stretch receptors are largely responsible for the signal to the brain to release more oxytocin, causing stronger contractions, which in turn helps bring that lower uterine segment up to build the fundus, opening the cervix more.
But in the second stage of labor, the star of the show is actually the pelvic floor, and specifically the nerves within that sling of muscles, and on the interior surface of the sacrum. We have to remember and understand that muscles respond to stimuli, meaning pressure sensation, on the nerves with contraction or relaxation.
We also must understand that there are several types of nerves, relating to the central (sensory) and autonomic (sympathetic and parasympathetic) nervous system. Each of these have a unique function and effects on the hormonal response in the brain.
Additionally, every womban is going to have slightly different nerve pathways, as we all have variations in our anatomy. So no womban will have the same experience of pleasure or pain in her pelvic area.
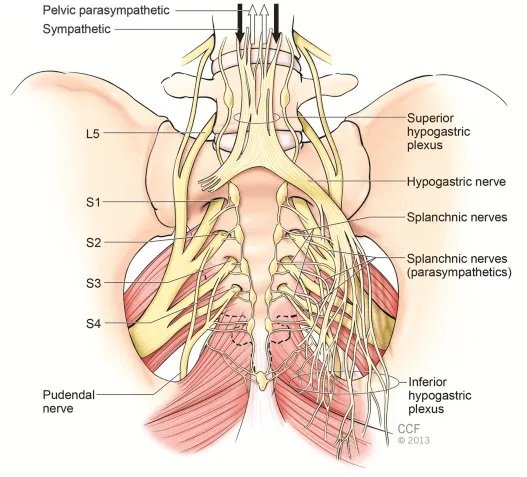
The primary nerves of the pelvis that are the stars of this show, are the pudendal nerves, which are mixed sympathetic, motor and sensory nerve fibers that wrap around the perineum, anus, and clitoris, and the pelvic splanchnic nerves which are parasympathetic fibers that emerge from the interior of the sacrum, as well as the sacral sympathetic splanchnic fibers.

When our body has finished pulling up the lower uterine segment, also known as “cervical dilation”, the baby either immediately or soon after drops down to the level of the ischial spines. At this point, there is a very important, often overlooked, cardinal movement that the baby makes, again sometimes instantly, sometimes after hours of pause. This is the internal rotation of the head to clear the ischial spines, letting the head through this narrow landmark in the middle of the pelvis, allowing it to then fully drop to meet the pelvic floor musculature and nerves, and the perineum, for crowning.
Here is a look from below at this bony landmark. Do you see the points facing inward? These are the ischial spines. Can you see how it would be hard for the baby’s head to go further in this position? This is why we need this moment of pause called the Quietude or Rest and Be Thankful stage after dilation, and before “pushing”, to allow the baby to navigate this landmark and drop fully.

“The second stage is defined as the stage when the cervical dilatation is full. However, the second stage diagnosis must include the fetal head position at ischial spine at level zero according the ACOG classification. The diagnosis of fetal head (FH) position in the birth canal is performed by traditional vaginal digital examination (VE) and recently by intrapartum ultrasound (IU) also. The diagnosis of second stage based only on cervical dilatation is incomplete and requires the diagnosis of FH in the birth canal.” (1)
This is a really important distinction to understand, and while this may seem like a very dense subject so far, I want you to have enough understanding of your anatomy and the physiology of birth to be able to understand the following point:
If we begin pushing just because a womban is fully dilated, rather than confirming that the baby is not only at the “zero station” at the ischial spines, but actually that the baby’s head has rotated to get past the ischial spines, we are making a grave mistake. The result is that a womban may push and push and push for long hours, while the baby remains stuck on those spines, unable to rotate and drop fully down into the pelvic floor.
We also may find that the act itself of pushing before the Fetal Ejection Reflex kicks in, may override the sensitive neurological signals coming from the nerves of the pelvic floor.
Here is the main point I want every birthing person to understand:
A healthy fetal ejection reflex is going to be more achievable if we create the right environment. It is long understood from the experiments done by Constance Benyon and Michel Odent that if we give womben enough time, most will end up having a physiologically self-directed pushing stage, perhaps even with a strong FER.
Even in the following research in 2004 and 2020 we found an important correlation between a woman feeling safe in labor, and the hormone cascade. If a womban feels scared, threatened, or the environment simply doesn’t foster peace, the body will send stress hormone catecholamine, which will slow down the labor and inhibit FER even in a healthy womban. (2)(3)
Fostering an environment of safety, non-disturbance, and patience is crucial.
What I think is missing from some of this earlier research is that we also need to consider some of the other factors at play in individual womben’s anatomy.
Our pelvic floor function is going to be individual to our unique body and life experience. In our current paradigm, most of us spend more time sitting than we are designed for, and historically, indigenous humans have spent more time walking, squatting, and changing activities throughout their day. This alone is going to change how our body behaves, and how our pelvic and other muscles work.
Then there are additional factors such as tailbone traumas, other accidents or injuries, excessive weakness due to lifestyle factors, inflammation or even simple muscular imbalances due to imbalanced movement patterns in life or workouts.
These imbalances can cause muscles to become weak on one side, and tense on another. They can cause impingement of nerves within muscle fibers that have been caught in tension patterns. Muscles can also be both tight and weak at the same time, because that tension pattern prevents them from contracting or releasing fully. And all of these factors can contribute to inflammation in the muscle and nerves.
The result in these cases is the potential for more pain in labor, as well as potentially causing the baby to descend in an imbalanced manner, putting undue stress on one side or another, and on the nerves in a particular part of the pelvis. Even a tight psoas muscle on one side may be a factor in the way the baby lays in the uterus and descends into the birth canal.
And, when the baby drops into the nerve-rich musculature of the pelvic floor, including onto the sacrum with its interior covered in nerves, including the parasympathetic splanchnic nerves, this pressure, when evenly applied to a healthy, unobstructed nervous system, can cause the cascade we call the Fetal Ejection Reflex.
The parasympathetic and sympathetic nerves receive this pressure sensation, sending signals to the brain to both open and relax, while also creating a surge of oxytocin and adrenaline for a series of profoundly strong contractions which cause this immense, involuntary bearing down sensation.
It is my clinical hypothesis, which I have witnessed in my work as a bodyworker, that impingement on these nerves due to tailbone, pelvic floor or sacral traumas and imbalances, can augment this FER. This may potentially inhibit a healthy nerve response, interrupting that potential cascade leading to FER, and oftentimes also correlating with increased pain.
But I’m not going to leave you hanging here!
There are very profoundly helpful things you can do to ensure a healthy pelvic response prior to or during pregnancy.
A combination of pelvic floor release work done either at home (as I teach in my online courses) or by a professional, along with pelvic floor physical therapy as needed for a tailored approach, and/or pelvic floor and general exercises like I teach in my program, can go a long way to ensuring we enter the birthing tides in balance. We need to be able to address areas of tension and holding patterns first, and then look at how we move, breathe, and exercise, second. This combined approach is, in my opinion, the core of childbirth preparation which needs to be given more consideration in our modern era.
I am doing my best to address this gap in our education, one person at a time. To learn more, and delve deeper into this subject and my expertise on this, visit https://nourishedwatersbirth.com and join my cohort of amazing womben learning all about their bodies and babies in the birth and postpartum continuum. Even if you have had a history of painful labors, long second stage, or trauma, you can take action here and now to heal, recover, and potentially prepare for another baby in the best way possible. I hope to see you there!
1.) Antonio Malvasi et al. Oxytocin augmentation and neurotransmitters in prolonged delivery: An experimental appraisal. European Journal of Obstetrics & Gynecology and Reproductive Biology. March 2024. Available online at https://www.sciencedirect.com/science/article/pii/S2590161323000996
2.) Ibone Olza et al. Birth as a neuro-psycho-social event: An integrative model of maternal experiences and their relation to neurohormonal events during childbirth. PubMed 2020. Available online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386571/
3.) Judith A Lothian, Do Not Disturb: The Importance of Privacy in Labor; PubMed 2004. Available online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1595201/